-
Special topic on this only.
-
Flu vaccines have reduced the risk of flu-associated hospitalizations among older adultsexternal icon on average by about 40%.
A 2018 studyexternal icon that included influenza seasons from 2010-2016 showed that getting a flu shot reduced a pregnant woman’s risk of being hospitalized with flu by an average of 40 percent
https://www.cdc.gov/flu/vaccines-work/vaccineeffect.htm
The flu vaccine for the 2018–2019 season was only 29 percent effective.
But it is big optimism:
Immunized workers who do catch the flu, return to work half a day sooner on average.
Most probably most of them illegaly get to work during the night breaking windows.
The UK's Chief Medical Officer, Christopher Whitty, told a Parliamentary committee on Friday that there was "concerning" evidence suggesting that it may not be possible to stimulate immunity to the virus.
-
they're getting ready to give people something .... http://endoftheamericandream.com/archives/138-million-u-s-government-contract-will-accelerate-production-of-500-million-pre-filled-covid-19-vaccine-injection-devices
-
I don't think you can compare flu vaccine--the 40 percent figure never is quoted with the context. If say 5 percent get the flu, and you get the vaccine, you lower your risk from 5 percent to say 2 percent, or even 1.5 percent, your serious illness risk is real, of course, but way lower, you are in a very small percentile. Not to say you should not get the vaccine, of course, I get my vaccine. It's just that the numbers look bigger without the context of what the number is. OTOH, Covid could infect a whole lot of people, and even if you survive, you can have serious, long lasting complications. More like Polio, I think, possibly worse. Hope someone will come up with a solid vaccine.
-
Goal of this topic is that people need to understand is that vaccine is similar to bad masks.
Statistically it can change a lot, but in your specific case it is almost completely pointless.
As none of manufacturer warrant efficiency of vaccine in each specific case and for each of strains. Strangely, best vaccines results are reported for countries with widest masks usage :-)
We need real big number research with forced controlled infectioning, but no one want to do it, and it seems like guys have a reason.
Actually whole last year we could observe war on any people who questioned vaccine efficiency, and it was not clear why such big push happened. Now we perfectly know why Youtube, Facebook and alike prepared for almost a year.
-
Background. The 2014–2015 influenza season was distinguished by an epidemic of antigenically-drifted A(H3N2) viruses and vaccine components identical to 2013–2014. We report 2014–2015 vaccine effectiveness (VE) from Canada and explore contributing agent–host factors.
Methods. VE against laboratory-confirmed influenza was derived using a test-negative design among outpatients with influenza-like illness. Sequencing identified amino acid mutations at key antigenic sites of the viral hemagglutinin protein.
Results. Overall, 815/1930 (42%) patients tested influenza-positive: 590 (72%) influenza A and 226 (28%) influenza B. Most influenza A viruses with known subtype were A(H3N2) (570/577; 99%); 409/460 (89%) sequenced viruses belonged to genetic clade 3C.2a and 39/460 (8%) to clade 3C.3b. Dominant clade 3C.2a viruses bore the pivotal mutations F159Y (a cluster-transition position) and K160T (a predicted gain of glycosylation) compared to the mismatched clade 3C.1 vaccine. VE against A(H3N2) was −17% (95% confidence interval [CI], −50% to 9%) overall with clade-specific VE of −13% (95% CI, −51% to 15%) for clade 3C.2a but 52% (95% CI, −17% to 80%) for clade 3C.3b. VE against A(H3N2) was 53% (95% CI, 10% to 75%) for patients vaccinated in 2014-2015 only, significantly lower at −32% (95% CI, −75% to 0%) if also vaccinated in 2013–2014 and −54% (95% CI, −108% to −14%) if vaccinated each year since 2012–2013. VE against clade-mismatched B(Yamagata) viruses was 42% (95% CI, 10% to 62%) with less-pronounced reduction from prior vaccination compared to A(H3N2).
Conclusions. Variation in the viral genome and negative effects of serial vaccination likely contributed to poor influenza vaccine performance in 2014–2015.
-
We attribute the decline in influenza-related mortality among people aged 65 to 74 years in the decade after the 1968 pandemic to the acquisition of immunity to the emerging A(H3N2) virus. We could not correlate increasing vaccination coverage after 1980 with declining mortality rates in any age group. Because fewer than 10% of all winter deaths were attributable to influenza in any season, we conclude that observational studies substantially overestimate vaccination benefit.
-
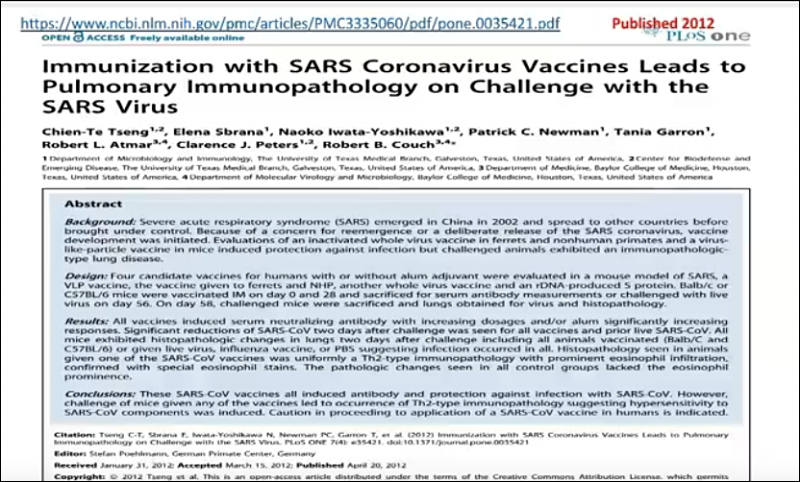
The formation of so-called "non-neutralizing antibodies" can lead to an exaggerated immune reaction, especially when the test person is confronted with the real, "wild" virus after vaccination. This so-called antibody-dependent amplification, ADE, has long been known from experiments with corona vaccines in cats, for example. In the course of these studies all cats that initially tolerated the vaccination well died after catching the wild virus.
The vaccinations are expected to produce antibodies against spike proteins of SARS-CoV-2. However, spike proteins also contain syncytin-homologous proteins, which are essential for the formation of the placenta in mammals such as humans. It must be absolutely ruled out that a vaccine against SARS-CoV-2 could trigger an immune reaction against syncytin-1, as otherwise infertility of indefinite duration could result in vaccinated women.
The mRNA vaccines from BioNTech/Pfizer contain polyethylene glycol (PEG). 70% of people develop antibodies against this substance -- this means that many people can develop allergic, potentially fatal reactions to the vaccination.
The much too short duration of the study does not allow a realistic estimation of the late effects. As in the narcolepsy cases after the swine flu vaccination, millions of healthy people would be exposed to an unacceptable risk if an emergency approval were to be granted and the possibility of observing the late effects of the vaccination were to follow. Nevertheless, BioNTech/Pfizer apparently submitted an application for emergency approval on December 1, 2020.
 sa15739.jpg785 x 501 - 100K
sa15739.jpg785 x 501 - 100K -
if you have problems with scribd, PDF here:
Wodarg Yeadon EMA Petition Pfizer Trial FINAL 01DEC2020
-
In 2021 and 2022 nothing will change
Because none of vaccines will be used for people above 60 and below 10 years during this time.
With coronavirus 90-97% of deaths are people above 60. And children are main virus spreaders always.
-
WHY PEOPLE WILL START DYING A FEW MONTHS AFTER THE FIRST MRNA "VACCINATIONS"
She sounds little nuts and mostly refers to antibody-dependent amplification, ADE.
https://video.wakkeren.nl/videos/watch/9bd9f602-e5e9-47e0-b35d-8f1bfd78f0f4
I strongly advice to check scientific papers on this all, instead of such videos.
 sa16119.jpg800 x 482 - 86K
sa16119.jpg800 x 482 - 86K -
Novavax, one of six US companies that received hundreds of millions of dollars upfront from the US government to develop a COVIID-19 vaccine, has just released preliminary data from its Phase 3 trials. The data showed the vaccine was 89.3% effective in the UK branch of the trial.
In a separate Novavax trial held in South Africa, the efficacy was significantly lower. In a small trial the rate of protection was just 50%. Almost all the cases that scientists have analyzed there so far were caused by the mutated strain, known as B.1.351.
New round of vaccines coming.
-
Richer members of the World Trade Organization (WTO) blocked a push by over 80 developing countries on Wednesday to waive patent rights in an effort to boost production of COVID-19 vaccines for poor nations.
https://www.reuters.com/article/us-health-coronavirus-wto-idUSKBN2B21V9
Who cares about the poor...the rich definitely not.
-
It can be very bad precedent for companies.
Poor countries must totally stop any medical related patents functioning on their territory.
-
What about Medicago vaccine? The institution I work is doing "voluntary" vaccination with this thing. However their site is full off difuse terms.
-
Fox allows Peter McCullough to tell the truth








Howdy, Stranger!
It looks like you're new here. If you want to get involved, click one of these buttons!
Categories
- Topics List23,990
- Blog5,725
- General and News1,353
- Hacks and Patches1,153
- ↳ Top Settings33
- ↳ Beginners256
- ↳ Archives402
- ↳ Hacks News and Development56
- Cameras2,366
- ↳ Panasonic995
- ↳ Canon118
- ↳ Sony156
- ↳ Nikon96
- ↳ Pentax and Samsung70
- ↳ Olympus and Fujifilm100
- ↳ Compacts and Camcorders300
- ↳ Smartphones for video97
- ↳ Pro Video Cameras191
- ↳ BlackMagic and other raw cameras116
- Skill1,960
- ↳ Business and distribution66
- ↳ Preparation, scripts and legal38
- ↳ Art149
- ↳ Import, Convert, Exporting291
- ↳ Editors191
- ↳ Effects and stunts115
- ↳ Color grading197
- ↳ Sound and Music280
- ↳ Lighting96
- ↳ Software and storage tips266
- Gear5,420
- ↳ Filters, Adapters, Matte boxes344
- ↳ Lenses1,582
- ↳ Follow focus and gears93
- ↳ Sound499
- ↳ Lighting gear314
- ↳ Camera movement230
- ↳ Gimbals and copters302
- ↳ Rigs and related stuff273
- ↳ Power solutions83
- ↳ Monitors and viewfinders340
- ↳ Tripods and fluid heads139
- ↳ Storage286
- ↳ Computers and studio gear560
- ↳ VR and 3D248
- Showcase1,859
- Marketplace2,834
- Offtopic1,320


